DOAC Switching Calculator
This calculator helps determine the safest time to switch from warfarin to a direct oral anticoagulant (DOAC) based on your current INR level, kidney function, and other health factors. Proper timing is critical to avoid dangerous bleeding or clotting risks.
Your Current Information
Critical Switching Guidelines
Important: The timing of your switch is critical. Switching too early can lead to dangerous bleeding. Switching too late can increase stroke risk.
Switching Timing Recommendations
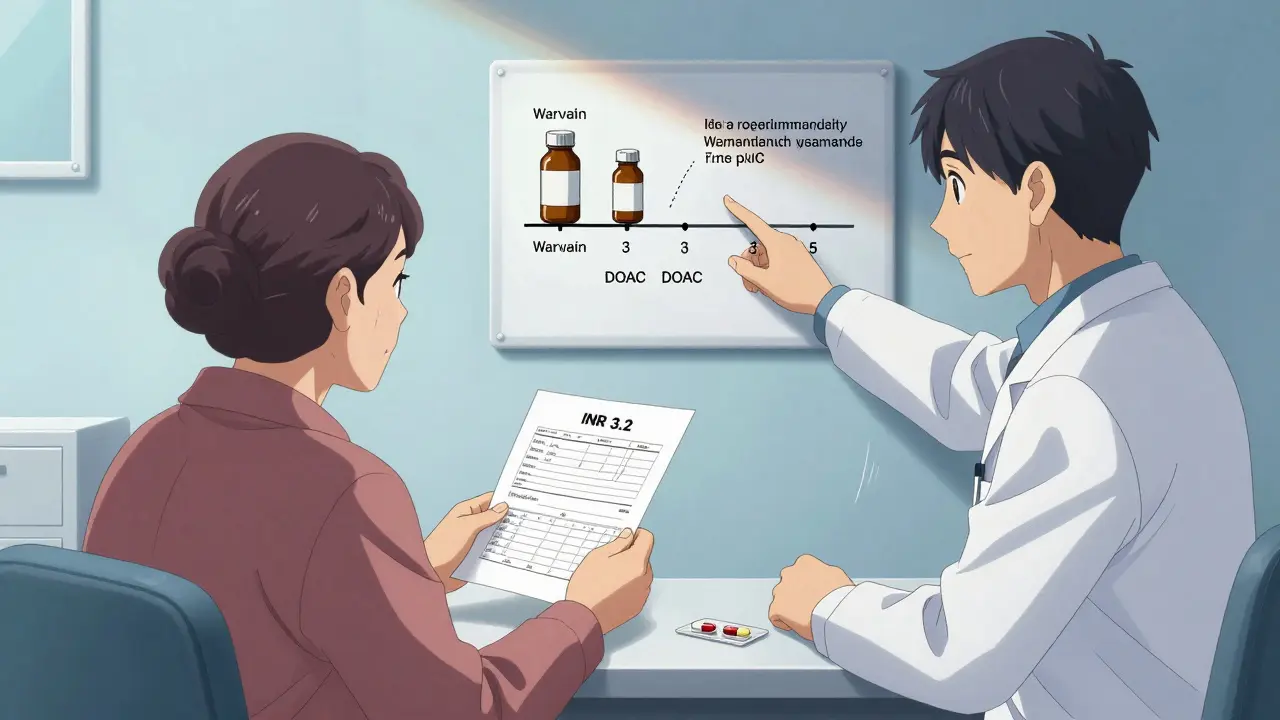
INR ≤ 2.0: Start DOAC immediately
INR 2.0-2.5: Start DOAC today or wait until tomorrow
INR 2.5-3.0: Wait 1-3 days, then recheck INR
INR ≥ 3.0: Wait 3-5 days, then recheck INR
Important Considerations:
- Mechanical heart valves: DOACs are not safe - stay on warfarin
- CrCl < 15 mL/min: DOACs may not be safe - discuss alternatives
- Weight < 60 kg or > 150 kg: May need dose adjustment
Results & Recommendations
Switching from warfarin to a direct oral anticoagulant (DOAC) sounds simple - no more weekly blood tests, fewer food restrictions, and less hassle. But if you skip the details, this switch can be dangerous. Thousands of people make this change every year, and while most do fine, others end up in the ER because the timing was off, the dose was wrong, or they weren’t screened properly. This isn’t about guessing. It’s about following clear, proven steps - and knowing what can go wrong.
Why Switch from Warfarin at All?
Warfarin has been the go-to blood thinner for over 70 years. It works, but it’s finicky. You need your INR checked every 1-4 weeks. Too high, and you risk bleeding. Too low, and you could get a stroke. You also have to watch what you eat. Leafy greens, cranberry juice, even some herbal supplements can throw off your dose. It’s a constant balancing act. DOACs - like apixaban, rivaroxaban, dabigatran, and edoxaban - changed that. They don’t need regular INR tests. They have fewer food interactions. And studies show they’re just as good at preventing strokes, with a lower risk of dangerous brain bleeds. The RE-LY trial found intracranial bleeding dropped from 4.0 to 2.7 per 100 patient-years when switching to dabigatran. That’s a big deal. But here’s the catch: DOACs aren’t magic. They don’t work the same way in everyone. And if you switch too soon or too late, you’re putting yourself at risk.When NOT to Switch
Not everyone should switch. Some people absolutely should stay on warfarin. Here are the red flags:- You have a mechanical heart valve. DOACs don’t work well here - they increase the risk of clots. Warfarin is still the only safe option.
- Your kidneys are failing. If your creatinine clearance (CrCl) is below 15-30 mL/min (depending on the DOAC), most of these drugs aren’t safe. Dabigatran, for example, is cleared mostly by the kidneys. If they’re weak, the drug builds up and you bleed.
- You have severe liver disease (Child-Pugh Class C). The liver helps break down DOACs. If it’s failing, the drugs stick around too long.
- You’re pregnant or breastfeeding. DOACs can cross the placenta and harm the baby. Warfarin is risky too, but it’s better studied in pregnancy - and sometimes still used under strict supervision.
- You weigh less than 60 kg or more than 150 kg. Most clinical trials didn’t include people at these extremes. We don’t know how well the standard doses work for you.
The Critical Timing Rules
This is where most mistakes happen. You can’t just stop warfarin one day and start a DOAC the next. You need to time it based on your last INR. Here’s what the American Heart Association and European Society of Cardiology agree on:- INR ≤ 2.0: Start the DOAC right away.
- INR 2.0-2.5: Start the DOAC today or wait until tomorrow.
- INR 2.5-3.0: Wait 1-3 days. Recheck your INR.
- INR ≥ 3.0: Wait 3-5 days. Recheck. Don’t start the DOAC until it drops.
DOAC-Specific Safety Notes
Not all DOACs are the same. Each has quirks.- Dabigatran: Must be kept in its original bottle. It’s moisture-sensitive. If you put it in a pill organizer, it can lose potency. Also, it’s taken twice a day - missing a dose matters more than with once-daily DOACs.
- Rivaroxaban: Should be taken with food. If you take it on an empty stomach, your body absorbs less. That means less protection against clots.
- Apixaban: Has the lowest risk of bleeding among DOACs. Often preferred for older adults or those with kidney issues.
- Edoxaban: Requires INR ≤ 2.5 before starting. Less forgiving than the others.
What About Side Effects?
DOACs have fewer side effects than warfarin - but they’re not side-effect-free.- Gastrointestinal bleeding: More common with DOACs than warfarin, especially in the first few weeks. If you notice black stools, vomiting blood, or even just new stomach pain - call your doctor.
- Kidney problems: DOACs are cleared by the kidneys. If your kidney function drops, the drug builds up. That’s why we check CrCl every 6-12 months - even if you feel fine.
- Drug interactions: Some antibiotics, antifungals, and seizure meds can raise DOAC levels. Always tell your pharmacist you’re on a blood thinner before starting anything new.
- Missed doses: DOACs have short half-lives. If you miss a dose, take it as soon as you remember - unless it’s close to your next one. Then skip it. Don’t double up. Missing even one dose can leave you unprotected.
Preparation Before the Switch
A good switch isn’t just about the day you change pills. It starts weeks before. Here’s what your doctor should check:- Your most recent INR (within the last 30 days).
- Your creatinine and liver function tests (from the last 6 months).
- Your weight - yes, even if you’ve weighed the same for years.
- Your medication list - including over-the-counter painkillers, supplements, and herbal teas.
- Your renal function using the Cockcroft-Gault formula - not just the lab’s eGFR.
What Happens After the Switch?
You’re not done after the first pill. You still need follow-up.- Check in with your doctor in 2-4 weeks. They’ll ask about side effects, adherence, and any new symptoms.
- Get your kidney function checked every 6-12 months. Even if you feel great.
- Carry your anticoagulant alert card at all times. Emergency rooms need to know you’re on a DOAC.
- Keep your DOAC in its original packaging. Especially dabigatran. Don’t dump it into a pill organizer unless your pharmacist says it’s safe.
- Know the signs of bleeding: unusual bruising, nosebleeds that won’t stop, red or brown urine, severe headaches, dizziness.
Cost and Access
Let’s be real: DOACs cost a lot. In the U.S., warfarin runs $10-$30 a month. DOACs? $500-$700. Insurance often covers them, but not always. Some patients skip doses because they can’t afford them. That’s dangerous. If cost is an issue, talk to your doctor. Ask about patient assistance programs. Some manufacturers offer free medication for those who qualify. Don’t stop taking it just because it’s expensive.What If You Need Surgery?
If you’re having a procedure - even a simple tooth extraction - your DOAC timing matters. Here’s what the British Columbia protocol says:- Low-risk procedure (like a dental cleaning): Hold dabigatran for 24 hours if CrCl >90 mL/min. Hold for 48 hours if CrCl is 30-50 mL/min.
- High-risk procedure (like knee replacement): Hold dabigatran for 96-108 hours if CrCl is 30-50 mL/min.
Final Thought: This Isn’t a DIY Decision
Switching from warfarin to a DOAC isn’t like changing your blood pressure med. It’s high-stakes. The guidelines are clear: only clinicians with anticoagulation experience should manage this transition. If your doctor hasn’t done this before, ask for a referral to a specialized anticoagulation clinic. Or ask your pharmacist - many now run anticoagulation services. They’re trained in these protocols. You’re not being difficult. You’re being smart. And in this case, smart saves lives.Can I switch from warfarin to a DOAC on my own?
No. Switching requires precise timing based on your INR level, kidney function, and other health factors. Doing it without medical supervision increases your risk of stroke or dangerous bleeding. Always work with a doctor or pharmacist trained in anticoagulation management.
Which DOAC is safest for older adults?
Apixaban is often preferred for older adults because it has the lowest risk of bleeding in clinical trials. It’s also less dependent on kidney function than dabigatran or edoxaban. But the right choice depends on your weight, kidney health, and other medications. Your doctor should calculate your CrCl and review your full profile before deciding.
Do I still need blood tests after switching?
You won’t need INR tests anymore, but you still need kidney function checks. Most guidelines recommend a blood test for creatinine every 6-12 months. If you have kidney disease, you may need them more often. Your doctor should schedule this - don’t wait until you feel sick.
Can I take aspirin or ibuprofen after switching?
Avoid NSAIDs like ibuprofen, naproxen, or high-dose aspirin unless your doctor says it’s okay. These drugs increase bleeding risk when combined with DOACs. Acetaminophen (Tylenol) is usually safe for pain relief. Always check with your pharmacist before taking any new OTC medication.
What if I forget to take my DOAC?
If you miss a dose and remember within 6-12 hours of when it was due, take it right away. If it’s been longer, skip the missed dose and take your next one at the regular time. Never double up. Missing doses increases your stroke risk - especially if you have atrial fibrillation. Set phone reminders or use a pill box with alarms.








LiV Beau
March 12, 2026 AT 00:01 AMI switched from warfarin to apixaban last year and honestly? Life changed. No more weekly finger pricks, no more worrying about spinach at dinner, and my doctor said my INR was stable for YEARS before the switch. I still get my kidney checked every 6 months, but that’s it. Also, I use a pill organizer with alarms - game changer. 🙌
Denise Jordan
March 12, 2026 AT 08:01 AMYeah right. Like DOACs are somehow safer. My cousin had a GI bleed and they said it was because of rivaroxaban. Now he’s back on warfarin and doing fine. This whole thing feels like Big Pharma pushing expensive pills.
Adam Kleinberg
March 13, 2026 AT 01:25 AMIve read the guidelines and theyre basically saying trust your doctor but dont trust the data because the trials were funded by manufacturers who make these drugs and if you think about it the whole warfarin vs DOAC debate is just a distraction from the real issue which is that our healthcare system is broken and people are being sold snake oil under the guise of medical progress
Gene Forte
March 13, 2026 AT 17:26 PMThis post is one of the clearest, most practical guides I’ve seen on anticoagulation transitions. It’s rare to find something this detailed without being overwhelming. The timing chart alone? Worth printing and taping to the fridge. We need more content like this - not just for patients, but for primary care docs who aren’t specialists. Thank you.
Kenneth Zieden-Weber
March 14, 2026 AT 04:38 AMI love how this breaks down the DOACs like a tech spec sheet. Dabigatran: moisture-sensitive. Rivaroxaban: needs food. Apixaban: the chill one. Edoxaban: the stickler. Honestly, if you treat these like you treat your phone’s battery settings - know the limits, don’t push them - you’ll be fine. Also, never skip a dose. Ever. I set three alarms. One on my watch, one on my phone, one on my smart speaker. I’m not risking a stroke because I overslept.
David L. Thomas
March 15, 2026 AT 09:28 AMThe renal clearance point is critical. I had a patient last month - 78, CrCl 28, on dabigatran. She didn’t know her kidney numbers had dropped. She ended up in the ER with a subdural. DOACs aren’t ‘easier’ - they’re just less visible in their risks. We need better patient education, not just better guidelines.
Mike Winter
March 17, 2026 AT 00:17 AMI appreciate the thoroughness here. Though I wonder if the cost barrier is being underplayed. In the UK, we have access through the NHS, but I know patients in the US who ration their meds because of price. That’s not a clinical issue - it’s a moral one. If we’re going to recommend these drugs, we need to make them accessible. Otherwise, we’re just writing prescriptions for privilege.
Randall Walker
March 17, 2026 AT 19:01 PMI mean... I get it. But I’ve seen too many people get scared by the word 'bleeding' and then stop taking their meds entirely. Like, yeah, GI bleed is bad. But stroke? Also bad. And way more common. So if you’re going to be scared, be scared of the right thing. Also, don’t take ibuprofen. Ever. Seriously. I’m not joking. Tylenol. That’s it.
Miranda Varn-Harper
March 19, 2026 AT 02:52 AMThe suggestion that patients should 'ask for a referral to an anticoagulation clinic' is both admirable and elitist. Most primary care practices don’t even have a pharmacist on staff. And in rural areas? There are no clinics. This advice assumes a level of healthcare access that simply does not exist for millions. It’s not helpful - it’s tone-deaf.
Alexander Erb
March 19, 2026 AT 22:56 PMI’m a pharmacist and I’ve helped over 200 people switch. The biggest mistake? Not checking the last INR. People think 'oh, I stopped warfarin last week' - but if their INR was 3.8 when they stopped? You’re playing Russian roulette. Also, always keep the original bottle. Dabigatran in a pill organizer? It’s like leaving your phone in the microwave. It doesn’t work. And yes, I’ve seen it happen. Twice.
Donnie DeMarco
March 21, 2026 AT 15:09 PMbro i just switched last month and i was terrified but like... honestly it’s been chill. no more blood tests, no more being weird at dinner, and my doc said my kidney numbers are solid. i take my apixaban with my morning coffee and i never forget. i even got a lil sticker on my fridge that says 'DOAC LIFE'. you’re welcome, future me 🤘
Tom Bolt
March 23, 2026 AT 03:15 AMI was on warfarin for 12 years. Then I switched. Then I had a hemorrhage. Then I went back. Then I had another. Then I sued. The system is rigged. The trials are biased. The drug reps are everywhere. And now? I’m just a walking warning label. Don’t trust the hype. Don’t trust the guidelines. Trust your gut. And if your gut says 'no' - don’t switch.
Shourya Tanay
March 24, 2026 AT 23:08 PMIn India, access to DOACs is extremely limited. Most patients still use warfarin due to cost. But even when DOACs are available, many doctors lack training. I’ve seen cases where patients were switched without renal assessment. It’s not negligence - it’s systemic lack of infrastructure. We need training programs, not just guidelines.